
1. Background
2. Why cardiac MRI is beneficial:
Cardiac MRI is well suited for the examination of an ASD because it can accurately quantify the shunt, and its effect on cardiac structure and function. It can directly visualize blood flowing across the ASD. It is totally non-invasive and does not require contrast.
3. . MRI technique:
Short and long axis SSFP images are obtained to quantify the end-diastolic and end-systolic volumes of both ventricles, and to determine global systolic function (LV and RV EF). Phase contrast images are acquired to quantify blood flow in the main pulmonary artery (Qp) and the ascending aorta (Qs) to determine the shunt ratio (Qp/Qs). For the most accurate results, an identically prescribed phase-contrast image of a stationary phantom is used for baseline correction of the flow data.
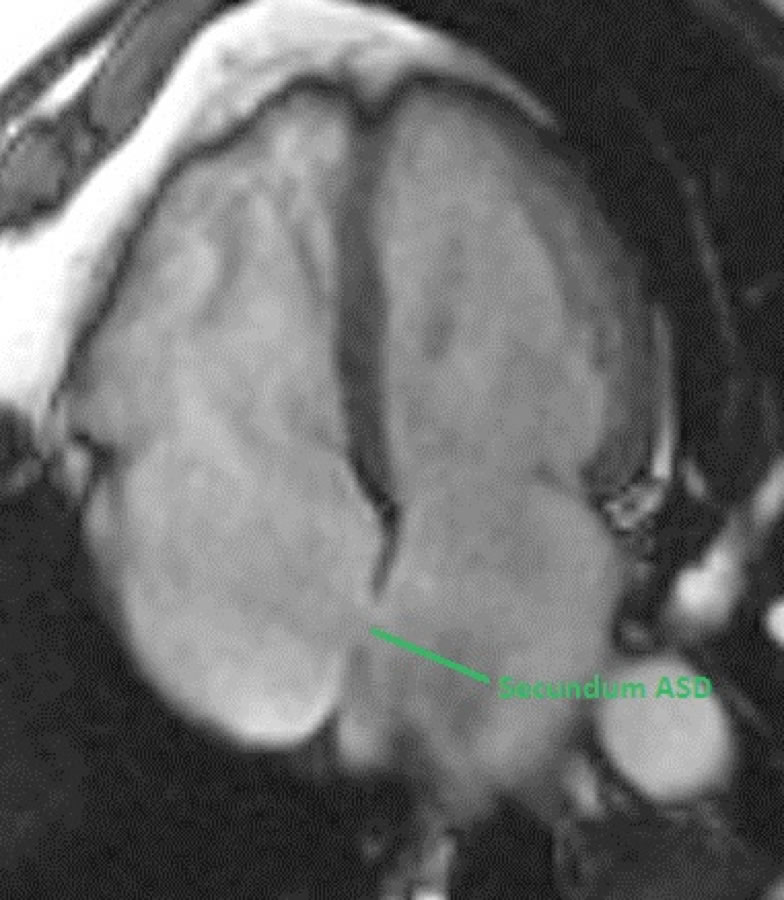
In order to make the specific diagnosis of atrial septal defect, one must visualize blood flowing directly between the atria. To visualize a defect in the interatrial septum, ECG-gated SSFP or fast gradient echo images are sometimes acquired perpendicular to the septum at the fossa ovals, typically as a stack of either 4-chamber images or short axis images (as shown in the image below).

click to enlarge
However, visualizing a defect this way is sometimes problematic, especially when the ASD is less than 1 cm in diameter (because of partial volume averaging with slices that are often ~8 mm thick). Furthermore, merely visualizing an apparent defect in the interatrial septum is insufficient to make a diagnosis unless blood can be seen flowing directly across the septum. Partial volume averaging can sometimes make it difficult to see an intact interatrial septum.
A more robust method for demonstrating a secundum ASD is to acquire phase-contrast images parallel to the septum at the level of the fossa ovalis. With this method, blood flow through the interatrial septum travels perpendicular to the imaging plane and easily detected.
IV. Analysis:
The best way to quantify the shunt ratio (Qp/Qs) is to divide the blood flow in the main pulmonary artery (Qp) by the blood flow in the ascending aorta (Qs). In the case of an isolated ASD (i.e. no other shunts or regurgitant valve disease), Qp should equal the RV stroke volume, and Qs should equal the LV stroke volume. Qp/Qs will be >1 in most cases because left atrial pressure typically exceeds right atrial pressure. However, in patients with pulmonary hypertension and right ventricular hypertrophy (i.e. Eisenmenger physiology), it is possible for the shunt to reverse and be predominantly right-to-left, resulting in a Qp/Qs < 1.0.
SSFP images showing a secundum ASD.

V. Which imaging findings affect treatment?
The severity of ASD can be quantified in terms of Qp/Qs and defect size. Percutaneous closure and surgery are generally reserved for patients with Qp/Qs > 1.5, unless they are undergoing cardiac surgery for other reasons.
VI. Drawbacks of existing tests:
Transthoracic echocardiography is most commonly used to assess for an ASD. Many patients also undergo transesophageal echocardiography for a better anatomic assessment. MRI is less invasive and is superior for quantifying the size of the shunt (Qp/Qs), as well as its affect on RV size and function. MRI is also good at identifying other possible associated anatomic abnormalities such as partial anomalous pulmonary venous return.

